The other day my wife noticed how I was preparing my skratch drink mix (ie. Adding scoop after scoop of the white drink mix to my water bottles), and she voiced a concern that all these high carb/sugary sport fuel products I consume, could be putting stress on my body, which might lead to type 2 diabetes.
I dismissed her concern, and explained that because I am burning through so much of those carbs/sugar when I ride, I don’t have anything to worry about. But am I right about that? I mean, I do consume a lot of energy gels, cliff bars, ounces of skratch/Gatorade mix, and various other sport fuel products, but at the same time, I train a lot too.
Perhaps us cyclists, and endurance athletes in general, who consume far more sugar than might otherwise be recommended, aren’t at risk of developing insulin resistance. But, could all these products be putting us at risk of some other gut ailment or nutritionally induced health issue?
I don’t think there are long term robust studies that show endurance athletes are immune to T2D. I know there is evidence that short term use is fine.
Somebody share with me the study if there is one. I think it’s just anecdotal.
I don’t think just because you’re exercising that you can drink sugar with impunity. However, it has a big effect on performance for endurance exercise, so the benefit outweighs the cost in the short run
I’m afraid this is just not correct. Glut4 requires insulin.
T1Ds decrease insulin because the work of cycling burns glucose, not because glucose magically gets into the cells - insulin is still required to open the cellular absorption pathway.
I would caution against saying everyone can drink sugar with reckless abandon and no one can drink sugar at all. We’re all different and have different physiology. I for example am prediabetic. I only have carbs / sugar when I’m cycling, rest of the time I’m zero carb. Cycling friends I know are able to consume sugar that would make me diabetic, whilst maintaining low HBA1Cs.
We’re all different. Best thing you can do is to have an impaired fasting glycemia test and an HBA1C and see where you are on the metabolic spectrum.
Where, then, is the glucose burned if not in the cells? Just going poof! in the blood?
No, it doesn’t require insulin. GLUT4 translocation is indeed stimulated by insulin. Insulin binds to the insulin receptor on the cell membrane, which dimerizes and catalyzes a signaling cascade whose net result is insertion of the GLUT4 transporter into the cell membrane. GLUT4 allows facilitated diffusion of glucose into the cell. The diffusion itself does not require insulin.
Muscle contraction (skeletal, cardiac) can, independent of insulin, cause insertion of the GLUT4 transporter into the cell membrane. Thus, glucose can be brought into the cell.
Unless this study actually correlates certain genes, the narrative just as validly suggests that nurture rather than nature plays the biggest role in development of T2DM. For example, mom and dad got fed junk by grandparents. They have the habit of eating junk. Raise their kids eating junk. Everyone develops T2DM. T2DM is considered a ‘lifestyle disease’.
Perhaps eating high amounts of sugar in a bike somehow has no direct effect on long term health. However, few people can consume high amounts of sugar without having it affect the palate. Few people can consume sugar only while on the bike. I imagine these people would develop T2DM in the long run. Some outlier elite athlete may not, but a typically weekend warrior hobby cyclist likely will
@redlude97
This is the punchline to that literature review:
“ While we know that a person’s future risk of developing T2D has a significant heritable component and believe that most of this inherited risk is associated with particular genotypic features (in most cases, multiple variants of small effect?), and have identified several risk variants in genome-wide association studies, these variants still explain a relatively small proportion of the observed heritability. Several studies have found that a risk score based on traditional risk factors (BMI, family history, age, sex, HDL, triglycerides, etc .) consistently outperforms any set of genetic markers and the addition of known genetic markers does not significantly improve prediction based on traditional risk factors[81-83].”
It seemed that many genes have been correlated but they never mention the extent to which their presence explains incidence of T2DM (because it is negligible). It is easy to find a statistically significant effect in science. It’s much harder to find one with a magnitude that is clinically meaningful. Sociodemographic and lifestyle factors currently do so given the state of the literature.
I highly doubt the average person would read that statement you quote above and feel that it is a jump to a conclusion. Though, I do think the conclusion is logical. Feel free to experiment and prove it wrong. I hope you stay T2DM free! Lol
Several studies have found that a risk score based on traditional risk factors (BMI, family history, age, sex, HDL, triglycerides, etc .) consistently outperforms any set of genetic markers and the addition of known genetic markers does not significantly improve prediction based on traditional risk factors[81-83].”
It is not surprising that “traditional risk factors” which include genetics indirectly (through family history) are not improved by adding genetic markers. You’ve basically already controlled out the effect.
Furthermore, the study showing that genetics was a large factor already controlled for age and weight, which are other known factors.
Anyway, consumption of sugar while exercising is definitely not a “traditional risk factor”. One of the studies you refer to has two such lists: Cambridge (age, sex, drug treatment, family history of type 2 diabetes, body mass index, smoking status) and Framingham (age, sex, parental history of type 2 diabetes, body mass index, high density lipoprotein cholesterol, triglycerides, fasting glucose). Neither has any dietary component. If consumption of sugar while exercising doesn’t spike your insulin levels (for reasons given above), and doesn’t cause weight gain (because you’re burning the calories at least as fast as you’re taking them in), there’s no obvious mechanism for it to cause Type 2 diabetes. And this applies to the weekend warrior as much as the top athlete, as long as the WW is not gobbling gels while sitting on the couch.
Kind of. But kind of also not quite. Cellular insulin sensitivity is 50x higher during exercise. Magnitude of insulin response in non-T1D folks is miniscule during exercise compared to outside of exercise.
This is important.
There is currently an over-application of T2D & T1D info to non-diabetics in the field of sport nutrition.
There isn’t. And there is serious physiological mechanistic reason to believe that people with blood sugar dysregulation can indeed consume high levels of sugar during exercise and pose no risk of pancreatic damage.
As an anecdote, this past spring I consumed 300-700g of sugar per day for almost a month and ended up with an a1c of 4.9.
If there were risk, my wife and I, and probably @brendanhousler would have extremely high likelihood of being diabetic by now. As a great sport science professor of mine usually asked when folks asked about health risks where there were none, “where are the bodies!?!” (as in, where are the bodies of athletes dropping dead from T2D). Yes, it’s totally crass, and insensitive and inappropriate but it highlights an important point:
Where there is risk, there will be some correlation, at least. There isn’t here.
PS. don’t ask my wife about her dental health.
Couldn’t have said it better myself. Saving this response!
I still don’t buy that Glut4 works in the absence of insulin. I do agree that we are more insulin sensitive when exercising, but insulin is required to open the door. The links posted above seemed to prove my point.
I think one of the biggest benefits of exercise is the increased insulin sensitivity after exercise has completed - for a period of up to about 36 hours I think based on what I have seen looking at my constant glucose monitor when I’ve used them.
Again, I think it comes down to genetic predisposition - some people are just a lot more prone to T2D, and yes, you still get T2Ds with BMI of 21 so if you’re worried, best thing is to have yourself tested as I describe above.
@Dr_Alex_Harrison… 300-700grams of sugar a day is crazy! 700grams of sugar is about 2,800 calories which is a LOT to burn. Glad you have a low HBA1C but for sure I’d never ever do this since I’ve become aware of my predisposition to T2D.
My point is that there is a behavioral aspect to it. High sugar intake for a recreational athlete may be harmless in the moment, but I know plenty of once great cyclists that are overweight or obese now because their habit of eating continued when their serious training stopped.
I’m suggesting that the median recreational cyclist likely doesn’t have the discipline to stop the sugar when they ride less or stop because of habit formations. Taste buds and the brain get desensitized to sugar. It just doesn’t immediately revert when your training goes down. There are plenty of studies showing how salty and sugary food are addicting and how overeating is a psychological/ mental health problem.
I agree that sugar improves endurance performance, but it is not a cost less benefit. There is always a trade off, that’s just the way life is. So that said, it might not be worth it for an average recreational cyclist to consume sugar as if they’re riding in the TdF because the benefit may not meet the cost
Glut4 translocation from inside cell to outside cell is well substantiated to be caused by two things:
insulin
Muscle activity.
As long as you’re burning what you consume, when you consume it, there is no known risk.
I add the word “known” purely out of respect that we as humans do not foresee the future. But in non-researcher-speak… there is no risk.
Bingo.
A human body is a masterful thing at seeking homeostasis.
And I would never ever recommend it to someone with current or past blood sugar dysregulation. Just to be clear!
I’d posit that endurance athletes who become obese after their endurance career ends probably become so because of an unhealthy restrictive tendency for which the “on” switch was finally shut off.
If we collected data on these folks, I’d bet there is an inverse correlation between hourly fuel intake reported during pro endurance career, and pounds gained after career.
I posit it actually works in their favor. Drinking sugar water on bike → habituation of drinking sugar water on bike. Remove bike, remove sugar water habituation.
NOT drinking sugar water on bike → habituation of “eat everything in the fridge, off the bike.” Remove bike, habituation to eat everything in the fridge still exists.
100% correct. Did an experiment once. At 600g carbs post-workout, via frosted flakes. By the end of the mixing bowl of frosted flakes, they tasted like corn chips in milk. Can confirm!
It does, if it’s constrained to on-bike.
It does not if it’s not constrained to on-bike.
Yes. Overeating. Not drinking sugar-salt-water on bike.
We agree. No truer words. There are no solutions. Only tradeoffs.
We disagree. In fact, increasing, and then optimizing, sugar-salt-water consumption has been one of the primary ways I’ve been able to help endurance athletes lose weight and improve blood panel results. So much so that I made a couple memes about it.
I was surprised too, at first. Until it became such a reliable pattern that I could not get clients, no matter how thoughtful and well-written the rest of the diet plan was, to eat appropriate kcal around the clock, if they were under-fueling training.
Turns out, hypoglycemia during and after training has lingering hunger effects hours after kcal needs have been caught up on. Hypoglycemia also leads to reduced activity intensity, duration, and if experienced regularly, it leads to habitually reduced frequency of training, eventually.
Since body composition issues and inactivity, and not sugar consumption during and only during exercise, are the leading predictors of T2D, it turns out that I can make a very strong case that increasing, then optimizing, sugar consumption during training, actually prevents T2D in the endurance athlete population.
“optimizing” = somewhere between 0-140g/hr, depending on duration, intensity, body comp history, satiety needs, total weekly volume, + a dozen other things.
PPS. Many folks still did not lose weight. Weight loss and future maintenance is intensely challenging. I’m not saying “drink more sugar and you’ll definitely lose weight.” Just pointing out a compelling correlation that is a large “n” to counterpoint “sugar during exercise causes problems.” I posit that when done optimally, it solves more health problems than it causes.
Agree with @Dr_Alex_Harrison on this one. I used to under fuel on bike then in the hours post ride was starving and eat anything and everything, usually junk! Now I fuel much more during the workout (just usually with sugar water and some squash for flavour) and do 20 mile runs or 3hr rides and come back and pretty much just eat normal (even though still calorie deficit at 90-100g sugar an hour). Just nowhere near as hungry so now just eat pretty constantly off the bike regardless of training (fairly stable and healthy diet) since on bike/run fuel so much more.
I no longer take in extra carbs on the bike on rides less than 2hrs. Unless you have a monster FTP and are doing >2hr rides, the math says you should be able to eat 2-3meals a day sufficiently to maintain expenditure or have a slight deficit without much challenge.
I’ve done the >100g bottles before and while I was fast (3.8w/kg and 314ftp) I was always insatiable 30min after getting off the bike. Since switching the intense hunger no longer occurs and I’m much happier for it
Yeah, I see a trend towards folks wanting to use >90g/hr for 1-2hr rides, and I think in 90% of cases, that’s inadvisable. In >50% of cases, much much less is better for shorter & easier rides.
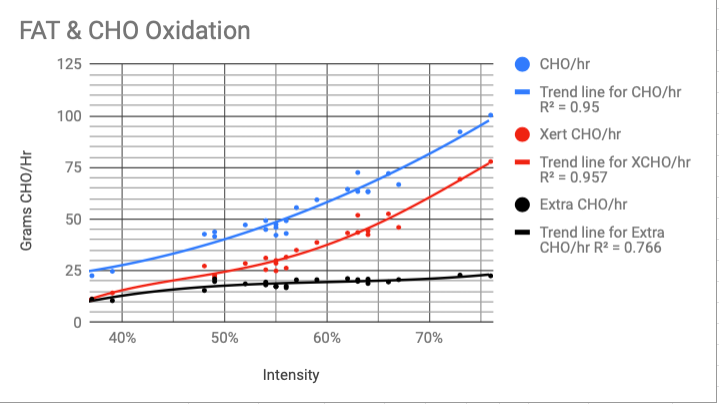
Couldn’t agree more. I’ve alternated over the years from eating next to nothing to stuffing myself with carbs and in the process got myself totally confused as to what and how much to eat. Just prior to the pandemic I had a metabolic test done and to see what my FAT & CHO burning was. I’ve finally used that data to produce a spreadsheet where I’ve split my rides into the 5 zones and applied the average fat burning in g/min to those zones, added up the total fat burned and converted it into calories. In that way I get an estimation of the carbs burned on the ride. With an FTP of 226W I’ve found that on my Endurance rides I burn between 40 & 60g of CHO/hour depending on the intensity of the ride. I use the XERT Fat/Carb Garmin app on the bike and found that it under reports the CHO by a consistent 20/25g hr which I can obviously account for (I suspect the discrepancy is due to my particularly low efficiency in converting chemical energy to mechanical <20%)
Yes, since I’ve started to be more specific about fueling on the bike, I’ve been eating much more healthily, less processed foods off the bike, without the excuse of eating junk to fuel.
It’s helped my training, helped me loose the menopause belly, supported my immune system.