Obviously talent - you can’t make a silk purse out of a sow’s ear but Drugs and/or Luck?
Just pointing out that there are multiple alternative explanations for what you offered as “evidence”.
Maybe because the method works, but his idea of why it works is wrong.
I won’t be splitting hairs on what the term significant means for you and what not. I appreciate the post, though ![]()
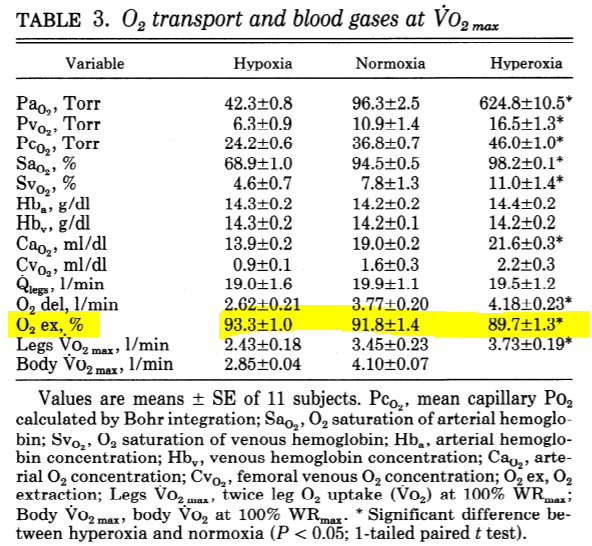
No need to split hairs, the data are clear: at VO2max, roughly 90% of the oxygen in arterial blood has been extracted by the exercising muscles, i.e., only about 10% remains.
Here is an example from 11 healthy, moderately-fit young men studied in hypoxia, normoxia, and hyperoxia. As highlighted, oxygen extraction is around 90% under all three conditions.
Please feel free to transfer insignificant 10% of your salary to me ![]()
All $1200 is yours. Where should I send it?
Help me reconcile that with what I posted above:
and

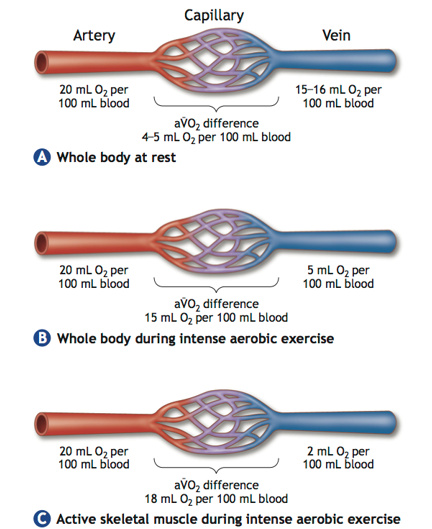
@empiricalcycling already alluded to this. The arteriovenous O2 difference is greater when measured across the exercising limbs compared to that measured across the whole body. That’s because even during maximal exercise, some blood is being sent to tissues (e.g., kidneys, skin) that don’t extract nearly as much O2 as the exercising muscles themselves.
IOW, venous O2 content is higher when measured in the pulmonary artery versus, e.g., the femoral vein because the former is “contaminated” with relatively O2-rich blood.
ETA: Here is the figure from McArdle, Katch, and Katch corresponding to one you found online.
![]() I love this forum!
I love this forum!
Sorry, seeing this a bit late, but interesting conversation. Hope I can still contribute.
Very general suggested explanation: that’s where most of the metabolic activity is occurring, ie. the greatest disruption to metabolic milieu, and subsequently the greatest signals back to your brain that “something is wrong down there” ![]() =
= ![]()
I haven’t seen much investigation into why or when someone might feel leg-limited vs breathing-limited. Would be interested if anyone else has. But I was surprised to see how much variability TR users were reporting in that other thread a while ago.
This adds to the greater point about local vs systemic a-vO2 differences. The microvasculature closest to/within the tissues where O2 is being utilized will obviously have greater O2 extraction and greater a-vO2 diff than tissues further away. If femoral vein a-vO2 diff is ~90%, I would guess that approaches 100% within the microvasculature, before ‘contamination’ from other less metabolically active tissues being drained into the femoral vein. eg. blood volume coming from skin and fat tissue, which is mostly still oxygenated.
I’m with you here. VLamax is a very convenient tool that appears to quantify phenotype well. But I’m skeptical how literally true or at least relevant the VLa measurement is to anything.
It’s up to us though to build on the VLamax model and/or make something that works better in the lab and on the road. Not just tear it down and walk away, IMO.
This isn’t what’s happening here. I’d love to admit that it were but if we take this mistake as true, then it has training implications that will not be borne out as effective. Oh right, and are not borne out by even the most basic understanding of the literature.
The book is just as cryptic. I was really disappointed by it. Grady appears to have some interesting ideas, but the book is poorly structured and lacks any real practical takeaways, IMHO.
100% agree. It’s like she only wrote half of it. It has some great explanations and ideas in. Then just ends before you have anything actionable that you can do. It’s all held back.
It’s like an advertisement to her coaching.
@Mikael_Eriksson To revive this old thread as I continuously come back to it… After some year now and a lot more experience… How do you think about these concept? Are you still categorizing training in VO2Max and VlaMax or is your “philosophy” more nuanced than that or maybe even simpler? Dan Lorang still seems to use this philosophy with great success.
As a recently self coached athlete for myself I believe in threshold work on the run and doing more work above threshold on the bike and rather race-specific in the swim. So currently in a VO2Max block where I still do (upper) threshold on the run as I think high intensity on the run is just not enough bang for the buck. But probably would make sense to intermix a VO2Max block after ~4-5 weeks with ~2 weeks of threshold work? Like some strength endurance and sweetspot work on the bike then going back into another ~4 weeks block of VO2Max? Anecdotally it has felt like threshold or also lactate clearance work have “solidified” gains in the VO2Max area into the threshold if that makes sense?
Anyway, I’d love an updated perspective here from you ![]()
I seem to recall that he no longer uses Insycd testing. I believe there are comments to be found on twitter if you search for vlamax.
My take is that the whole vlamax thing is a red herring and in the end, the Inscyd test is just an expensive power profile.
VLaMax is an interesting topic. I spent a long time trying to understand Mader and his model. I’m still I’m still trying to understand.
What I noticed from more than a dozen VLaMax tests in both running and cycling is that there’s a max lactate concentration associated with ending an effort for me. Whether it’s a 15 second effort or a 10 minute time trial, I’ll start around 1.0mmol/l and fail around 9-9.5 mmol/l, so about 8-8.5 delta.
But I can get my lactate concentration up to 16-18 mmol/l with repeated sprints before I give up completely. So for a single effort, there’s a lactate ceiling…a maximum lactate production. But at this point I’m not sure how to use that info.
That would be a maximal blood lactate concentration, not a maximal rate of lactate production.
Yes, you’re right.
Im missing a lot of the picture since I don’t know physiology. To me the similar concentration at failure is interesting.
I’m still not understanding what max production rate has to do with anything (rhetorically). Why was that so important to Mader?
The model put forward by Mader and Heck made an assumption that when linearly increasing exercise intensity, ADP concentration increases at a predictable and obligatory rate which would activate glycolytic throughput in kind. This is the first of three incorrect assumptions because it ignores training status, as countless studies (some available at the time) show that endurance training improves markers of mitochondrial enzyme concentration and oxidative ATP production, which in turn reduces the rate of ADP and AMP formation with better preserved muscle glycogen while improving fat oxidation. Or as The Cog says, glycolysis is sucked, it doesn’t “blow”, meaning it’s not made at an obligatory rate. The second incorrect assumption is that lactate/pyruvate is shuttled into the Krebs cycle first and preferentially, meaning fatty acids and ketone bodies are only used due to insufficient lactate formation. Again, we can see this is not true because diet can manipulate substrate availability and relative oxidation rates without a change in mitochondrial mass or enzyme density due to training status. A tangential assumption (let’s call it 2a) is that increasing vo2max is one of two ways to improve lactate oxidation, however the model leaves out the fact that improving training status means greater lactate oxidation even without an increase in vo2max, which violates the model’s assumption that lactate oxidation rate is the primary determinant of FTP. Further reading (predating the Mader & Heck paper by several years): https://journals.physiology.org/doi/pdf/10.1152/jappl.1984.56.4.831
The theoretical backing of the model is basically dead at this point, but now we get to the kicker and the answer to your question.
The reason all this matters is the third incorrect assumption, and is the second way to theoretically improve FTP. If glycolysis were activated at an obligatory rate, then it might be possible to raise or lower this rate to increase/decrease the production of lactate by modulating (via training) the fastest rate at which someone can make lactate (which also adds large error to this measurement since we are measuring blood lactate and making assumptions about equilibration between compartments, hydration, etc). This last assumption is incorrect because the people who make lactate the fastest have the best sprint because lactate production is a reaction to the ATP usage determined by such high work rates. You could improve your sprint power with better technique and change no other characteristics about your muscles or training status, and in theory you would have increased VLamax but in reality you haven’t as you just increased rate of ATP demand which is too rapid to be met by oxidative phosphorylation, or as Cog might say, the rate at which glycolysis is sucked. The model would say that if your FTP hasn’t changed but your sprint power and lactate formation goes up, your VO2max would necessarily have to have improved and this is measurably not true. Now we get to the last and probably most incorrect thing that’s kinda in the model but mostly in the training methodologies put forth by the model proponents, which is that whether or not we’re oxidizing lactate is what determines FTP. Lactate formation is not really a causal factor here, it’s a byproduct of whether or not energy state can be propped up via oxidative phosphorylation. So not only are the model’s most fundamental underlying assumptions all incorrect, the implications for training are generally also incorrect.


The above figures are from the 1988 Mader & Heck paper and probably the easiest visual aid in understanding the assumptions in the model.